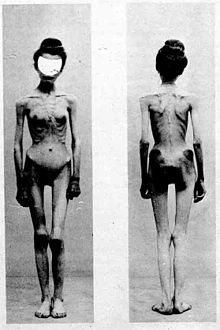
Anorexia nervosa, often referred to simply as anorexia,[11] is an eating disorder, characterized by low weight, food restriction, fear of gaining weight and a strong desire to be thin.[1] Many people with anorexia see themselves as overweight even though they are, in fact, underweight.[1][2] They often deny that they have a problem with low weight.[3] They weigh themselves frequently, eat small amounts and only eat certain foods.[1] Some exercise excessively, force themselves to vomit, or use laxatives to lose weight.[1] Complications may include osteoporosis, infertility and heart damage, among others.[1] Women will often stop having menstrual periods.[3] In extreme cases, people with anorexia who continually refuse significant dietary intake and weight restoration interventions, and are declared incompetent to make decisions by a psychiatrist, may be fed by force under restraint via nasogastric tube[12] after asking their parents or proxies[13] to make the decision for them.[14]

The cause is currently unknown.[2] There appear to be some genetic components with identical twins more often affected than fraternal twins.[2] Cultural factors also appear to play a role, with societies that value thinness having higher rates of disease.[3] Additionally, it occurs more commonly among those involved in activities that value thinness, such as high-level athletics, modeling and dancing.[3][4] Anorexia often begins following a major life-change or stress-inducing event.[3] The diagnosis requires a significantly low weight.[3] The severity of disease is based on body mass index (BMI) in adults with mild disease having a BMI of greater than 17, moderate a BMI of 16 to 17, severe a BMI of 15 to 16, and extreme a BMI less than 15.[3] In children a BMI for age percentile of less than the 5th percentile is often used.[3]
Treatment of anorexia involves restoring a healthy weight, treating the underlying psychological problems and addressing behaviors that promote the problem.[1] While medications do not help with weight gain, they may be used to help with associated anxiety or depression.[1] Different therapy methods may be useful, such as cognitive behavioral therapy or an approach where parents assume responsibility for feeding their child known as Maudsley family therapy.[1][15] Sometimes people require admission to a hospital to restore weight.[7] Evidence for benefit from nasogastric tube feeding, however is unclear;[16] such an intervention may be highly distressing for both anorexia patients and healthcare staff when administered against the patient's will under restraint.[12] Some people with anorexia will just have a single episode and recover while others may have recurring episodes over years.[7] Many complications improve or resolve with regaining of weight.[7]
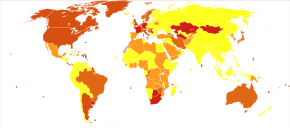
Globally, anorexia is estimated to affect 2.9 million people as of 2015.[9] It is estimated to occur in 0.9% to 4.3% of women and 0.2% to 0.3% of men in Western countries at some point in their life.[17] About 0.4% of young women are affected in a given year and it is estimated to occur ten times more commonly among women than men.[3][17] Rates in most of the developing world are unclear.[3] Often it begins during the teen years or young adulthood.[1] While anorexia became more commonly diagnosed during the 20th century it is unclear if this was due to an increase in its frequency or simply better diagnosis.[2] In 2013 it directly resulted in about 600 deaths globally, up from 400 deaths in 1990.[18] Eating disorders also increase a person's risk of death from a wide range of other causes, including suicide.[1][17] About 5% of people with anorexia die from complications over a ten-year period, a nearly six times increased risk.[3][8] The term "anorexia nervosa" was first used in 1873 by William Gull to describe this condition.[19]
Signs and symptoms
Causes
Mechanisms
Diagnosis
Treatment
Prognosis
AN has the highest mortality rate of any psychological disorder.[8] The mortality rate is 11 to 12 times greater than in the general population, and the suicide risk is 56 times higher.[22] Half of women with AN achieve a full recovery, while an additional 20–30% may partially recover.[8][22] Not all people with anorexia recover completely: about 20% develop anorexia nervosa as a chronic disorder.[114] If anorexia nervosa is not treated, serious complications such as heart conditions[20] and kidney failure can arise and eventually lead to death.[136] The average number of years from onset to remission of AN is seven for women and three for men. After ten to fifteen years, 70% of people no longer meet the diagnostic criteria, but many still continue to have eating-related problems.[137]
Alexithymia influences treatment outcome.[129] Recovery is also viewed on a spectrum rather than black and white. According to the Morgan-Russell criteria, individuals can have a good, intermediate, or poor outcome. Even when a person is classified as having a "good" outcome, weight only has to be within 15% of average, and normal menstruation must be present in females. The good outcome also excludes psychological health. Recovery for people with anorexia nervosa is undeniably positive, but recovery does not mean a return to normal.[medical citation needed]
Complications
Anorexia nervosa can have serious implications if its duration and severity are significant and if onset occurs before the completion of growth, pubertal maturation, or the attainment of peak bone mass.[138][medical citation needed] Complications specific to adolescents and children with anorexia nervosa can include the following: Growth retardation may occur, as height gain may slow and can stop completely with severe weight loss or chronic malnutrition. In such cases, provided that growth potential is preserved, height increase can resume and reach full potential after normal intake is resumed.[medical citation needed] Height potential is normally preserved if the duration and severity of illness are not significant or if the illness is accompanied by delayed bone age (especially prior to a bone age of approximately 15 years), as hypogonadism may partially counteract the effects of undernutrition on height by allowing for a longer duration of growth compared to controls.[medical citation needed] Appropriate early treatment can preserve height potential, and may even help to increase it in some post-anorexic subjects, due to factors such as long-term reduced estrogen-producing adipose tissue levels compared to premorbid levels.[medical citation needed] In some cases, especially where onset is before puberty, complications such as stunted growth and pubertal delay are usually reversible.[139]
Anorexia nervosa causes alterations in the female reproductive system; significant weight loss, as well as psychological stress and intense exercise, typically results in a cessation of menstruation in women who are past puberty. In patients with anorexia nervosa, there is a reduction of the secretion of gonadotropin releasing hormone in the central nervous system, preventing ovulation.[140] Anorexia nervosa can also result in pubertal delay or arrest. Both height gain and pubertal development are dependent on the release of growth hormone and gonadotropins (LH and FSH) from the pituitary gland. Suppression of gonadotropins in people with anorexia nervosa has been documented.[141] Typically, growth hormone (GH) levels are high, but levels of IGF-1, the downstream hormone that should be released in response to GH are low; this indicates a state of “resistance” to GH due to chronic starvation.[142] IGF-1 is necessary for bone formation, and decreased levels in anorexia nervosa contribute to a loss of bone density and potentially contribute to osteopenia or osteoporosis.[142] Anorexia nervosa can also result in reduction of peak bone mass. Buildup of bone is greatest during adolescence, and if onset of anorexia nervosa occurs during this time and stalls puberty, low bone mass may be permanent.[143]
Hepatic steatosis, or fatty infiltration of the liver, can also occur, and is an indicator of malnutrition in children.[144] Neurological disorders that may occur as complications include seizures and tremors. Wernicke encephalopathy, which results from vitamin B1 deficiency, has been reported in patients who are extremely malnourished; symptoms include confusion, problems with the muscles responsible for eye movements and abnormalities in walking gait.
The most common gastrointestinal complications of anorexia nervosa are delayed stomach emptying and constipation, but also include elevated liver function tests, diarrhea, acute pancreatitis, heartburn, difficulty swallowing, and, rarely, superior mesenteric artery syndrome.[145] Delayed stomach emptying, or gastroparesis, often develops following food restriction and weight loss; the most common symptom is bloating with gas and abdominal distension, and often occurs after eating. Other symptoms of gastroparesis include early satiety, fullness, nausea, and vomiting. The symptoms may inhibit efforts at eating and recovery, but can be managed by limiting high-fiber foods, using liquid nutritional supplements, or using metoclopramide to increase emptying of food from the stomach.[145] Gastroparesis generally resolves when weight is regained.
Cardiac complications
Anorexia nervosa increases the risk of sudden cardiac death, though the precise cause is unknown. Cardiac complications include structural and functional changes to the heart.[146] Some of these cardiovascular changes are mild and are reversible with treatment, while others may be life-threatening. Cardiac complications can include arrhythmias, abnormally slow heart beat, low blood pressure, decreased size of the heart muscle, reduced heart volume, mitral valve prolapse, myocardial fibrosis, and pericardial effusion.[146]
Abnormalities in conduction and repolarization of the heart that can result from anorexia nervosa include QT prolongation, increased QT dispersion, conduction delays, and junctional escape rhythms.[146] Electrolyte abnormalities, particularly hypokalemia and hypomagnesemia, can cause anomalies in the electrical activity of the heart, and result in life-threatening arrhythmias. Hypokalemia most commonly results in anorexic patients when restricting is accompanied by purging (induced vomiting or laxative use). Hypotension (low blood pressure) is common, and symptoms include fatigue and weakness. Orthostatic hypotension, a marked decrease in blood pressure when standing from a supine position, may also occur. Symptoms include lightheadedness upon standing, weakness, and cognitive impairment, and may result in fainting or near-fainting.[146] Orthostasis in anorexia nervosa indicates worsening cardiac function and may indicate a need for hospitalization.[146] Hypotension and orthostasis generally resolve upon recovery to a normal weight. The weight loss in anorexia nervosa also causes atrophy of cardiac muscle. This leads to decreased ability to pump blood, a reduction in the ability to sustain exercise, a diminished ability to increase blood pressure in response to exercise, and a subjective feeling of fatigue.[147]
Some individuals may also have a decrease in cardiac contractility. Cardiac complications can be life-threatening, but the heart muscle generally improves with weight gain, and the heart normalizes in size over weeks to months, with recovery.[147] Atrophy of the heart muscle is a marker of the severity of the disease, and while it is reversible with treatment and refeeding, it is possible that it may cause permanent, microscopic changes to the heart muscle that increase the risk of sudden cardiac death.[146] Individuals with anorexia nervosa may experience chest pain or palpitations; these can be a result of mitral valve prolapse. Mitral valve prolapse occurs because the size of the heart muscle decreases while the tissue of the mitral valve remains the same size. Studies have shown rates of mitral valve prolapse of around 20 percent in those with anorexia nervosa, while the rate in the general population is estimated at 2–4 percent.[148] It has been suggested that there is an association between mitral valve prolapse and sudden cardiac death, but it has not been proven to be causative, either in patients with anorexia nervosa or in the general population.[146]
Relapse
Rates of relapse after treatment range from 9–52% with many studies reporting a relapse rate of at least 25%.[96] Relapse occurs in approximately a third of people in hospital, and is greatest in the first six to eighteen months after release from an institution.[149]
Epidemiology
Anorexia is estimated to occur in 0.9% to 4.3% of women and 0.2% to 0.3% of men in Western countries at some point in their life.[17] About 0.4% of young females are affected in a given year and it is estimated to occur three to ten times less commonly in males.[3][17][149] Rates in most of the developing world are unclear.[3] Often it begins during the teen years or young adulthood.[1]
The lifetime rate of atypical anorexia nervosa, a form of ED-NOS in which the person loses a significant amount of weight and is at risk for serious medical complications despite having a higher body-mass index, is much higher, at 5–12%.[150]
While anorexia became more commonly diagnosed during the 20th century it is unclear if this was due to an increase in its frequency or simply better diagnosis.[2] Most studies show that since at least 1970 the incidence of AN in adult women is fairly constant, while there is some indication that the incidence may have been increasing for girls aged between 14 and 20.[17] According to researcher Ben Radford who wrote in Skeptical Inquirer "I found many examples of flawed, misleading, and sometimes completely wrong information and data being copied and widely disseminated among eating disorder organizations and educators without anyone bothering to consult the original research to verify its accuracy". Radford states that misleading statistics and data have been ignored by organizations like the National Eating Disorder Association who has not released data for "incidence of anorexia from 1984–2017" he states that each agency continues to report incorrect numbers assuming that someone else has checked the accuracy.[151]
Underrepresentation
Eating disorders are less reported in preindustrial, non-westernized countries than in Western countries. In Africa, not including South Africa, the only data presenting information about eating disorders occurs in case reports and isolated studies, not studies investigating prevalence. Data shows in research that in westernized civilizations, ethnic minorities have very similar rates of eating disorders, contrary to the belief that eating disorders predominantly occur in white people.[medical citation needed]
Men (and women) who might otherwise be diagnosed with anorexia may not meet the DSM IV criteria for BMI since they have muscle weight, but have very little fat.[152] Male and female athletes are often overlooked as anorexic.[152] Research emphasizes the importance to take athletes' diet, weight and symptoms into account when diagnosing anorexia, instead of just looking at weight and BMI. For athletes, ritualized activities such as weigh-ins place emphasis on weight, which may promote the development of eating disorders among them.[citation needed] While women use diet pills, which is an indicator of unhealthy behavior and an eating disorder, men use steroids, which contextualizes the beauty ideals for genders.[50] In a Canadian study, 4% of boys in grade nine used anabolic steroids.[50] Anorexic men are sometimes referred to as manorexic.[153]
History
The term "anorexia nervosa" was coined in 1873 by Sir William Gull, one of Queen Victoria's personal physicians.[19] The history of anorexia nervosa begins with descriptions of religious fasting dating from the Hellenistic era[154] and continuing into the medieval period. The medieval practice of self-starvation by women, including some young women, in the name of religious piety and purity also concerns anorexia nervosa; it is sometimes referred to as anorexia mirabilis.[155][156]
The earliest medical descriptions of anorexic illnesses are generally credited to English physician Richard Morton in 1689.[154] Case descriptions fitting anorexic illnesses continued throughout the 17th, 18th and 19th centuries.[157]
In the late 19th century anorexia nervosa became widely accepted by the medical profession as a recognized condition. In 1873, Sir William Gull, one of Queen Victoria's personal physicians, published a seminal paper which coined the term "anorexia nervosa" and provided a number of detailed case descriptions and treatments.[157] In the same year, French physician Ernest-Charles Lasègue similarly published details of a number of cases in a paper entitled De l'Anorexie hystérique.[158]
Awareness of the condition was largely limited to the medical profession until the latter part of the 20th century, when German-American psychoanalyst Hilde Bruch published The Golden Cage: the Enigma of Anorexia Nervosa in 1978. Despite major advances in neuroscience,[159] Bruch's theories tend to dominate popular thinking. A further important event was the death of the popular singer and drummer Karen Carpenter in 1983, which prompted widespread ongoing media coverage of eating disorders.[160]
Etymology
The term is of Greek origin: an- (ἀν-, prefix denoting negation) and orexis (ὄρεξις, "appetite"), translating literally to a nervous loss of appetite.
| This article uses material from the Wikipedia article Metasyntactic variable, which is released under the Creative Commons Attribution-ShareAlike 3.0 Unported License. |